Is Polyvagal Theory Debunked? What the 2026 Research Debate Means for Neurodivergent Nervous Systems
The 2026 Grossman critique challenges PVT's biology, but what does this mean for neurodivergent people who use polyvagal language? An honest breakdown with alternatives.
If you've been using polyvagal theory language to understand your nervous system, if you've told yourself "I'm in dorsal" during shutdown or "my ventral is offline" when you can't engage socially, the past few months might have felt destabilizing. A 39-author expert evaluation published in February 2026 declared the theory "untenable." And depending on which corner of the internet you landed in afterward, you either heard "PVT is pseudoscience, throw it all out" or "this changes nothing, the tools still work, relax."
Neither of those is quite right. And almost nobody is talking about the part that matters most to neurodivergent people.
So if you haven't come across polyvagal theory before, here's the short version. It was developed by Stephen Porges in the mid-1990s, and it proposes that your autonomic nervous system operates in three states: a "ventral vagal" state where you feel safe and socially engaged, a sympathetic fight-or-flight state, and a "dorsal vagal" shutdown state. It became massively popular in the trauma therapy world, partly through Deb Dana's books and what's known as the "polyvagal ladder." You'll find it referenced in Bessel van der Kolk's The Body Keeps the Score, in Gabor Maté's work, and in a huge range of therapy, yoga, and somatic practices. It gave clinicians and their clients a shared language for nervous system states, which is a big part of why it spread so fast.
What Grossman et al. actually argued
In February 2026, psychophysiologist Paul Grossman and 38 co-signatories published "Why the Polyvagal Theory is Untenable" in Clinical Neuropsychiatry. These aren't random skeptics. They're researchers with decades of collective expertise in vagus nerve physiology, neuroanatomy, vertebrate evolution, and autonomic function. Their argument targets several of PVT's core biological claims.
Here are the things they challenged:
The two-pathway claim. PVT says the vagus nerve has two distinct branches (dorsal and ventral) that function as separate systems with different evolutionary origins and different roles. Grossman et al. argue that while these anatomical branches exist, they don't function as independently or as neatly as PVT describes. The actual neuroanatomy is more distributed and overlapping than the clean "dorsal = shutdown, ventral = social engagement" model suggests.
The RSA measurement claim. PVT treats respiratory sinus arrhythmia (the natural variation in heart rate that occurs with breathing) as a reliable index of "vagal tone," and by extension, of your capacity for social engagement. Grossman has been challenging this for about two decades, and the 2026 paper continues to argue that RSA doesn't reliably measure what PVT says it measures. Too many other factors influence it. Barbier, Chen & Huizinga wrote a paper, published in Frontiers in Psychiatry in 2022 that's independent from this critique and shows most autistic children exhibit normal parasympathetic baseline values, which contradicts PVT's autism predictions and supports Grossman's evidence. You can find this study here.
The evolutionary narrative. PVT proposes a specific evolutionary sequence: reptiles had only the dorsal vagal system, mammals evolved the ventral vagal system for social engagement, and this phylogenetic hierarchy determines how our nervous system responds to threat. Grossman et al. argue that comparative physiologists have contradicted this narrative for decades, and that reptilian autonomic systems are more complex than PVT acknowledges.
The neuroception claim. PVT's concept of "neuroception" (the idea that your nervous system subconsciously evaluates safety and threat) is presented as a specific neural mechanism. The critique argues this remains a descriptive concept without the specific neural circuitry Porges claims for it.
The Social Engagement System. PVT describes a specific neural circuit linking the ventral vagus to facial muscles, middle ear muscles, and vocal prosody, forming a "Social Engagement System" that activates when you feel safe. The critique questions whether this system functions as a unified circuit in the way PVT describes.
These aren't minor technical quibbles, and the fact that 38 out of 39 invited domain experts agreed to co-sign says something about where the field stands on this. They target the biological foundation that the entire theory rests on.
What Porges responded
Stephen Porges published a rebuttal in the same journal issue. In it, he argues that Grossman et al. misrepresent PVT by attacking a simplified version of the theory, that PVT operates at a different "level of analysis" than the cellular neurophysiology his critics focus on, and that the critique doesn't meet the standard required for scientific refutation.
Some of these points land. Porges is right that popular presentations of PVT (the "polyvagal ladder," the colour-coded charts on Instagram) oversimplify the original theory, and it's fair to ask critics to engage with the actual published work. He also raises legitimate questions about what level of biological detail a clinical framework needs to provide.
Where the response falls short is in addressing the specific neuroanatomical and evolutionary challenges directly. Grossman et al. make concrete claims about vagal nerve anatomy and reptilian physiology with decades of comparative research behind them, and Porges's response often reframes these as misunderstandings of the theory's scope while leaving the specific evidence largely unaddressed.
There's also a broader pattern worth noting. In a March 2026 email to Polyvagal Institute students, I'm on that list and received the message, Porges referenced a forthcoming "canonical paper" that would address the scientific challenges comprehensively. As of this writing, Porges has not published that paper so I cannot link to the reference yet. The email's framing leaned heavily on procedural concerns (how the critique was organized, who signed it, whether the journal process was adequate, and whether the critique met formal consensus standards) and on delegating the scientific response to institutional affiliations while the biology itself went largely unaddressed.
This matters because practitioners and students who trained in PVT are looking for direct answers, and procedural deflection (regardless of whether the procedural concerns are valid) doesn't resolve the biological questions.
What this means for the tools you actually use
The part that gets lost in the polarized coverage is this: practical tools can work even when the theoretical explanation for why they work turns out to be wrong.
Slow breathing really does affect your autonomic state, and feeling safe in the presence of a regulated person really can shift your nervous system. Noticing whether your body feels mobilized, settled, shut down, or somewhere in between is genuinely useful information. Co-regulation is a real, documented phenomenon. These observations predate PVT and stand independently, and they don't require PVT's specific biological claims to be correct.
The problem is specificity. A practitioner who says "this exercise tones your ventral vagal nerve" is making a biological claim that PVT's contested anatomy can't actually support. A more accurate version would be something like "this exercise might help your nervous system shift toward a calmer state," which describes what people report experiencing without claiming a specific mechanism (and honestly, that framing is just better science communication anyway).
If you've been using polyvagal language to describe your internal states, you don't need to throw that vocabulary away overnight. "I feel shut down" and "I feel mobilized" are descriptions of real experiences. You can keep using them as descriptions while recognizing that the specific nerve-pathway explanation behind them is contested.
The part of this debate that's missing: PVT and neurodivergent nervous systems
Almost every piece written about this debate in 2026, from clinician blogs to Psychology Today columns, the Trauma Therapist Institute's response, and a growing number of Substack posts, speaks to a general therapy audience. Nobody is addressing what this debate means specifically for neurodivergent people. And it means quite a lot, because PVT has a neuro-inclusivity problem that goes beyond the biological critique.
PVT's "Social Engagement System" defines healthy regulation through neurotypical social cues: eye contact, facial expressivity, vocal prosody, and reciprocal social engagement. The ventral vagal state, the top of the polyvagal hierarchy, maps directly onto allistic social communication norms. If your nervous system's version of "regulated and safe" doesn't include sustained eye contact and conventional facial affect, PVT's framework reads you as being in a less regulated state. It pathologizes your baseline.
As Janae Elisabeth (Trauma Geek), a researcher-storyteller and neurodiversity advocate, has written in their neurodiversity paradigm analysis of PVT, throughout the PVT literature, the theory treats autism as equivalent to a deficit of function of the social engagement system, and positions restoring ventral vagal function as the path to "treating" autistic features. Trauma Geek names this "ventral supremacy": the assumption that being in ventral social engagement as often as possible is the goal, when stress responses are adaptive and many neurodivergent people regulate through means PVT doesn't recognize.
This framing shows up in PVT-adjacent education. Porges himself has taught continuing education courses co-administered through PESI that frame the work as understanding "deficits in the regulation of the Social Engagement System" as they "relate to the core features of autism." It's stated as such right in the course description.
To further quote the course outline, it also mentions "the severe social and emotional dysregulation of autistic individuals and a more optimistic narrative of minimizing these disruptive behaviors."
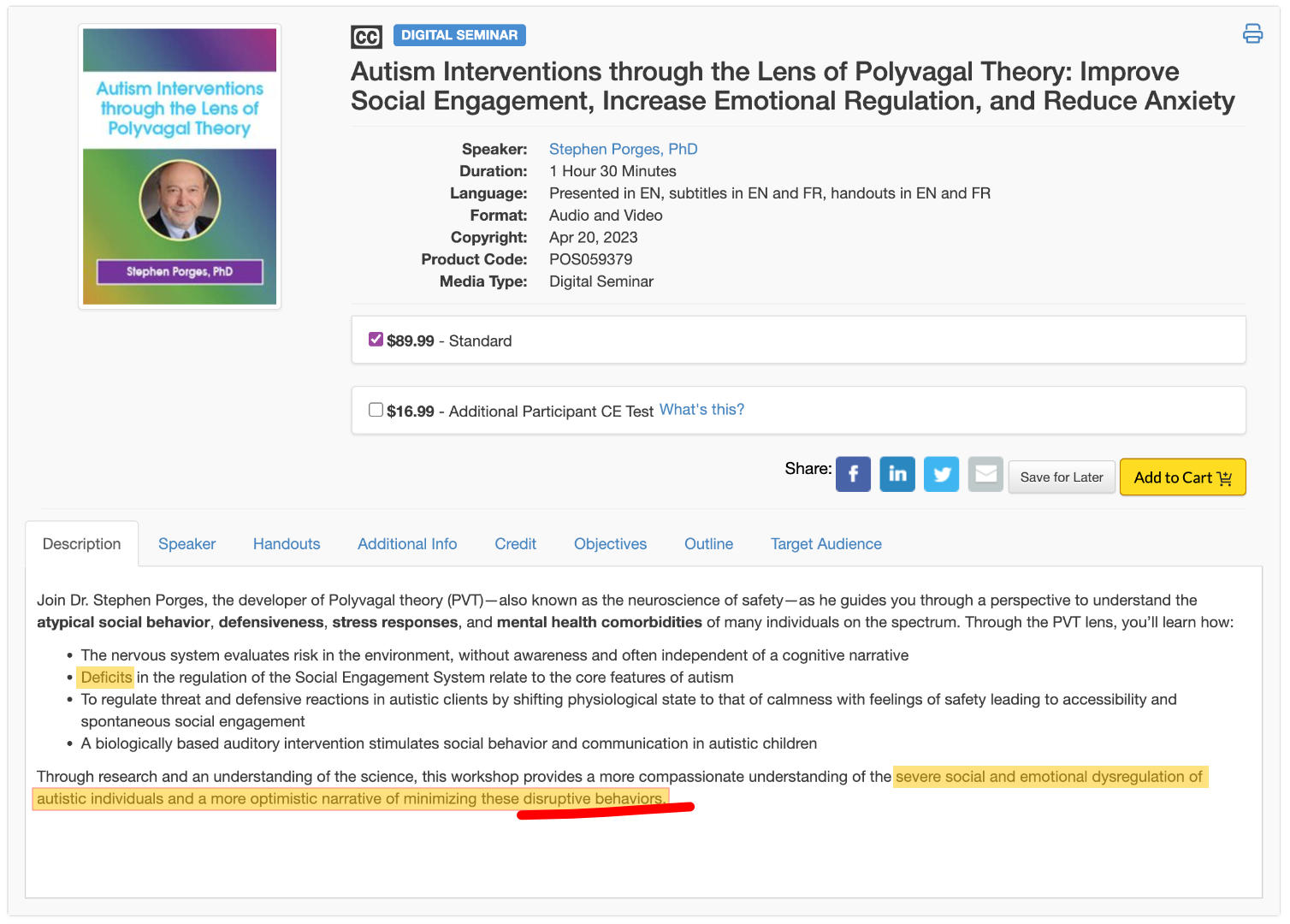
Excuse me while I go regulate my own nervous system after reading something so horrendously awful about our neurotype.
That language treats autism as a regulatory deficit to be corrected, something broken, and is of course deeply pathologizing regarding the way we communicate and socialize. Autistic people regulate differently, we communicate differently and perfectly fine with each other, and that difference is a feature of our neurology.
If our communication with allistic humans is a pathology, is a deficit, so is theirs with us. This is a deeply flawed and archaic model of neurodivergence.
And as an aside, the outcome of research using the "biologically based auditory intervention" (the same one mentioned in that course above, which is called the Safe and Sound Protocol or "SSP") has sustained criticism amongst adult autistic populations, including this overview from Trauma Geek and from Porges himself.
This was difficult to learn during the coursework I was presented with at the Polyvagal Institute after seeing PVT mentioned and used by so many reputable resources in the past, including autistic community resources, communities, and autistic therapists. The coursework was not presented as covering "neurodivergence" when it was brought up by another student, but the course materials included many references to autistic people and the overall positioning was that we were deficient. So it was a one-way conversation.
Materials on empathy and social cues were core aspects of the training, but all of them were framed in a way that emphasized that so-call deficiency. Our social cues were, essentially, a "threat" in communication and dysregulating to other humans.
I left the two first classes with severe jaw pain from the stress of masking in the manner we were instructed. I didn't notice I was doing it at the time because of interoception delay, but the pain started about an hour after class and repeated after the second class and both time lasted for over a day. We were told to keep our cameras on and to look engaged in a specific allistic way for the benefit of the instructors, and that was built into the actual coursework. I didn't experience this pain in other Zoom classes that were neuro-inclusive, for what it's worth. This is anecdotal, obviously, but it occurred.
When a theory's definition of "healthy" regulation maps exclusively onto neurotypical social behaviour, that theory can't adequately serve neurodivergent people. And when the biological foundation turns out to be wrong on top of that, the neurodivergent community has even less reason to keep using it as a primary framework.
What to use instead
If PVT's biology is contested and its framework actively pathologizes neurodivergent regulation, what do you actually use?
The Community Resilience Model (CRM) is the framework I prefer and use, and also teach. CRM focuses on six skills: Tracking (noticing body sensations without judging them), Resourcing (bringing to mind something that creates a sense of calm or strength), Grounding (using contact with the physical environment to stabilize), Gesturing (allowing the body's natural movements, I'll get into more detail in future resources), Help Now! (quick sensory-based stabilization activities), and Shift and Stay (gently moving your attention between what feels distressing and what feels okay in your body, then staying with the okay long enough for your nervous system to register it). These skills work at a practical, body-based level. What I tend to prefer is these skills don't depend on PVT's contested claims about dorsal and ventral vagal pathways, CRM's evidence base draws on the neuroscience of stress and resilience, and community-level biology education. It doesn't use the same biology as PVT in the training materials I went through, although for full transparency there was one mention of it informally by a trainer during the live coursework.
CRM uses the concept of a "Resilient Zone" (the range where your nervous system can handle stress and recover), which replaces PVT's polyvagal ladder hierarchy with something more flexible. When you're above the Resilient Zone (high zone), you might feel anxious and activated, on edge and restless. When you're below it (low zone), you might feel numb, flat, shut down, or disconnected. CRM's six skills help you move back into the zone where you can function. The Trauma Resource Institute designed it from the beginning as "appropriate technology" for community use by anyone, including people with zero clinical background. You can learn more about CRM through the Trauma Resource Institute and their iChill app.
Beyond CRM, several emerging frameworks offer more scientifically grounded explanations for the phenomena PVT tried to explain:
Predictive processing models describe your nervous system as constantly generating predictions about what's coming next and updating those predictions based on incoming sensory information. When the gap between prediction and reality gets too large, your system can become dysregulated. This framework can help explain why unpredictable environments are so costly for autistic nervous systems without pathologizing the nervous system itself.
Allostatic load refers to the cumulative wear on your body from chronic stress and repeated adaptation. For neurodivergent people who spend energy on masking, sensory management, operating in environments designed for neurotypical nervous systems, and recovering from all of that, allostatic load provides a concrete, measurable way to explain burnout that doesn't require any specific theory about vagal nerve branches.
The Neurovisceral Integration Model connects heart rate variability to prefrontal cortex function and emotional regulation in a way that's more empirically grounded than PVT's RSA claims. It provides a brain-body framework without the contested evolutionary hierarchy.
These frameworks are less catchy than "dorsal vagal shutdown" and that's partly why PVT spread so effectively (it told a simple, compelling story, and simple compelling stories travel fast). Accurate science is often more complex than that. But these alternatives can be explained accessibly, and they don't require you to accept biological claims that 39 authors of this paper say are wrong.
Where this leaves us
Polyvagal theory gave a lot of people, neurodivergent people especially, language for experiences that previously had no name. "I'm in dorsal" was a way to say "my body has shut down and I can't function right now" without having to call yourself lazy or broken or "just not trying hard enough." That matters, and losing the framework shouldn't mean losing the ability to describe what's happening to you.
The language can stay as description. The biology underneath it needs updating. And for neurodivergent people specifically, the new frameworks you choose should be ones that respect your nervous system's way of regulating as legitimate.
I'll be covering this topic in depth on Wired Divergent, my podcast and YouTube show about nervous system regulation for neurodivergent brains. If you want to read the full research document I've compiled on this debate, including the source verification, you can find it there.
FAQ
Q: Is polyvagal theory debunked?
A: A 39-author expert evaluation published in 2026 declared PVT's core biological claims
"untenable." The practical tools associated with PVT (breathing exercises, co-regulation, nervous
system state awareness, and somatic practices) can still be useful, but the specific biological
explanation PVT provides for why they work is seriously contested by domain experts.
Q: Can I still use polyvagal theory language?
A: You can use terms like "shutdown," "mobilized," and "settled" as descriptions of your internal
experience. Just be aware that these describe felt states, and the specific vagal nerve pathway
explanation behind them doesn't hold up under scrutiny from domain experts.
Q: Does polyvagal theory work for autism?
A: PVT has a neuro-inclusivity problem. Its Social Engagement System defines healthy regulation
through neurotypical social cues (eye contact, facial expressivity, vocal prosody, and reciprocal
social engagement), which can pathologize autistic communication and regulation styles. Frameworks
like CRM, predictive processing, allostatic load, and the Neurovisceral Integration Model provide
alternatives that respect neurodivergent regulation as legitimate.
Q: What is a good alternative to polyvagal theory?
A: The Community Resilience Model (CRM) offers practical, skills-based nervous system regulation
tools that don't depend on PVT's contested biology. For the scientific side, predictive processing,
allostatic load theory, and the Neurovisceral Integration Model offer more empirically grounded
explanations for the phenomena PVT tried to account for.